Umbilical Cord Blood in the Treatment of Myelodysplastic Syndrome
Myelodysplastic Syndrome (MDS) is a heterogeneous group of hematological disorders commonly characterized as a dysfunction of hematopoietic stem cells, leading to disordered production and inefficient blood formation in the bone marrow [1]. Typical manifestations of hematopoietic stem cell disorders include reduced peripheral blood cells, disorderly precursor cell differentiation, and increased or decreased bone marrow cells, with a high risk of transforming into Acute Myeloid Leukemia (AML) [2]. The incidence of MDS typically rises with age, affecting individuals over 60 years old at rates ranging from 6.7% to 33%, with a higher prevalence in males [3]. Due to the varying clinical presentations and disease progression, some patients may face lower survival chances upon diagnosis [4].
Prognosis and overall survival depend on several factors, such as the severity of cell depletion and the ratio of blood and marrow stem cells [2]. The widespread application of advanced sequencing technologies is rapidly advancing the understanding of the pathophysiology of Myelodysplastic Syndrome. However, allogeneic hematopoietic stem cell transplantation (HCT) derived from umbilical cord blood remains the only proven therapeutic method, showcasing the potential for recovery in some patients with improved disease status and survival post-HCT [4].
Characteristics of Myelodysplastic Syndrome
In healthy individuals, the bone marrow produces new, immature blood cells that mature over time [5]. Myelodysplastic Syndrome occurs when something disrupts this process, leading to the uncontrolled maturation of blood cells. Instead of developing normally, blood cells may die within the bone marrow or shortly after entering the bloodstream. Over time, there is an accumulation of immature and defective cells, causing health issues due to insufficient healthy red blood cells (anemia), infection due to a lack of healthy white blood cells (decreased leukocytes), and bleeding due to a shortage of platelets (decreased platelets) [6].
In-depth studies on the pathophysiology of Myelodysplastic Syndrome reveal various disease-causing factors [1]. Firstly, the incidence of MDS increases with age, with most cases occurring after 65 years and being most prevalent in patients over 80 years old, with a rate of 58 per 100,000 people, more commonly observed in males and individuals of Caucasian descent [10]. Some cases are associated with exposure to cancer treatments such as chemotherapy and radiation therapy, or toxic chemicals like benzene [7]. Reports suggest that sequence mutations largely contribute to the disease, with studies identifying one or more regulatory sequence mutations in 80% to 90% of common patients, including SF3B1, TET2, SRSF2, ASXL1, DNMT3A, RUNX1, U2AF1, TP53, and EZH2 [8]. For example, the RUNX1 mutation has been identified as disrupting the normal blood formation process.
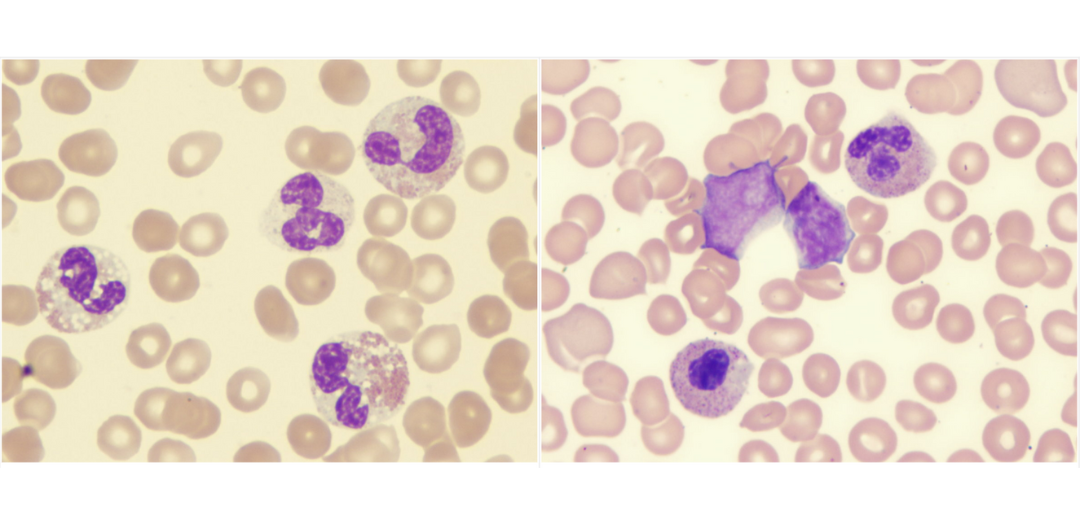
“Myelodysplastic-syndrome-dysplastic-eosinophils-demonstrating-abnormal-lobation-and-hypogranulation” and “Myelodysplastic-syndrome-showing-blast-and-monolobed-neutrophil”
Mutations have repeatedly occurred in over 100 genes in MDS, which encode spliceosome components, chromatin restructuring factors, model biosynthesis regulators, transcription factors, and many other factors [8]. The research findings indicate that these mutations correlate with various clinical features, including the degree of cell depletion, genetic cell transmission, and overall survival [1]. While gene mutations are not included in the prognostic system for MDS, they are believed to have an impact on the patient’s survival in some cases. For instance, TP53 is a tumor suppressor gene associated with a poorer prognosis compared to other mutations [9].
There are various types of Myelodysplastic Syndrome, primarily classified based on the disrupted blood components and their effects. These include single-lineage dysplasia syndrome, multilineage dysplasia syndrome, chromosome mutation-related myelodysplastic syndrome, and some unclassifiable cases with abnormalities in both morphology and DNA [5]. Despite efforts to develop drugs and treatment techniques for MDS, such as azacitidine or decitabine and chemotherapy [2], significant side effects have been observed in patients, including headaches, difficulty breathing, extreme fatigue, and potential reproductive issues [11].
Currently, allogeneic hematopoietic stem cell transplantation (HCT) is the sole therapeutic approach for Myelodysplastic Syndrome [12]. HCT offers the potential for curing Myelodysplastic Syndrome, primarily through robust immune-mediated responses against the tumor’s effects [13].
Blood Stem Cells and Umbilical Cord Blood Stem Cells Transplantation
For the majority of MDS patients, chemotherapy alone is often not a feasible treatment option. Only about 40% of patients experience disease remission, and it is usually short-lived [14]. For high-risk MDS patients, the 3-year survival rate after chemotherapy is only around 5% [15]. Currently, the only treatment with curative potential for MDS is Hematopoietic Stem Cell Transplantation (HSCT), with long-term survival rates ranging from 25% to 70% [16].
MDS originates from abnormal hematopoietic stem cells or precursor cells, and the goal of HSCT is to replace these cells and their offspring with cells from a healthy donor. Allogeneic HSCT requires 1) healthy donor cells for transplantation into the patient and 2) elimination or inactivation of disease-causing malignant cells [17]. Allogeneic Umbilical Cord Blood Stem Cell Transplantation (UCBT) offers the potential to cure Myelodysplastic Syndrome (MDS), primarily through immune-mediated suppression of tumor development combined with high-dose cell toxic therapies before transplantation [26]. This contrasts with other MDS therapies that may extend survival but do not eliminate the disease [1].
To ensure a successful transplantation process, doctors must suppress the patient’s immune system using immunosuppressive drugs, and T-cell and Natural Killer cell reactions mediate the body’s rejection of the graft. Continuous combination and testing of chemotherapy or radiation and evolving protocols are also necessary. The hurdle lies in HLA compatibility, as only 1/4 of patients have siblings who are HLA-matched antigens and older MDS patients with older siblings often seem unsuitable due to associated health conditions [17].
Bone Marrow Transplantation (BMT) is a viable candidate in HSCT but comes with numerous side effects, such as infections, graft rejection, and difficulty finding HLA-matched donors [18]. Hence, scientists have been exploring alternative sources.
Umbilical Cord Blood (UCB) collected from the umbilical cord and placenta after childbirth is a rich source of Hematopoietic Stem Cells (HSC) and serves as a substitute for bone marrow transplantation [1]. Umbilical Cord Blood Transplantation (UCBT) has become an accepted alternative donation source in cases where there is no suitable matched sibling or incompatible donor. Furthermore, research has proven that umbilical cord blood has superior cell components, quantity, and characteristics compared to bone marrow [19]. UCB has two distinctive advantages: a relatively high tolerance for HLA mismatch and the ability to be cryopreserved, making it readily available with flexible transplantation timing [20].
The application of appropriate cytokine combinations allows for the efficient development of various cell lineages from HSC obtained from umbilical cord blood [19]. This process finds application in medicine, particularly in the field of hematology. Hematopoietic stem cells in umbilical cord blood (CD34+CD38-) show stronger proliferation response to cytokines and are less dependent on supporting stromal cells than corresponding cells in bone marrow or peripheral blood [21].
In umbilical cord blood, hematopoietic progenitor cells with high proliferative potential (HPP-CFC) are present eight times more than in bone marrow [22]. The number of CD34+HLA-DR- and CD34+CD38- cells in umbilical cord blood is four times higher than in bone marrow [23]. Additionally, umbilical cord blood contains a higher proportion of primitive hematopoietic cells compared to bone marrow [24]. CFC analysis in umbilical cord blood reveals approximately 8,000 BFU-E (three times more than in bone marrow and peripheral blood) per 1 ml, ranging from 13,000 to 24,000 CFU-GM (15 times higher than in bone marrow and peripheral blood), and from 1,000 to 10,000 CFU-GEMM [25].
Umbilical cord blood stem cell transplantation in the treatment of Myelodysplastic Syndrome
In a study related to UCB transplantation in the treatment of myelodysplastic syndrome by Sato et al., significant recovery of neutrophils up to 90% on day 50 and platelet recovery of 88% on day 200 was observed in 33 patients who received a stem cell dose of 2.51×10^7 cells/kg [27]. The rates of acute and chronic GVHD in this study were 67% and 34%, respectively. However, the mortality rate post-transplantation and the relapse rate were around 14% and 16%, respectively, after five years. This clinical study demonstrated that UCBT could be considered for MDS patients in cases of compatible and incompatible HLA sources. Additionally, in this report, Sato emphasized that finding an 8/8 HLA-matched source in UCBT is a prerequisite for MDS treatment and reduces the risk of relapse or TRM later on.
CIBMTR, a collaborative research program of the Medical College of Wisconsin and the National Marrow Donor Program, includes a volunteer network of over 450 transplant centers worldwide, contributing detailed data on allogeneic and autologous transplant cases for statistics [28]. According to reports from 2004 to 2013, 176 adult MDS patients underwent umbilical cord blood transplantation (UCBT). In 80% of transplant cases, they used umbilical cord blood units with an average total nucleated cell (TNC) dose of 4 x 10^7 cells/kg. Results showed the cumulative recovery rates of neutrophils at 28 and 100 days after UCBT were 92% and 97%, respectively. The corresponding values for platelet recovery on days 28 and 100 were 66% and 86%, respectively. The cumulative rates of acute GVHD at day 100 were 38% and 14%, respectively. The probability of chronic GVHD after one year was 26% and 28%. Graft failure accounted for only 3% of deaths. However, the relapse rate post-transplantation reached up to 45%, suggesting that while the outcomes are somewhat promising, we need strategies to improve results for any donor source. UCB transplantation is the only assured source in treating MDS and provides better outcomes than BM combined with UCBT. The application of a wide range of disease treatment drugs, such as antioxidant drugs and lenalidomide, along with proactive supportive care, has contributed to better results for MDS patients over time [28]. Similarly, outcomes for patients undergoing allogeneic stem cell transplantation have improved, contributing to positive effects and the potential for disease recovery for MDS patients.
Umbilical Cord Blood Stem Cell Transplantation is currently the only proven method with the potential to cure the disease. Moreover, the development of public blood banks and the availability of umbilical cord blood have increased for a growing number of patients. Over 70% of patients report their quality of life as ‘good to excellent’ after transplantation [17]. With the availability of approved drugs for MDS treatment, ongoing research aims to combine various therapeutic agents to provide the best assistance for patients and strive toward complete recovery in the future.
References:
[1] DOTSON, Jennifer L.; LEBOWICZ, Yehuda. Myelodysplastic syndrome. In: StatPearls [Internet]. StatPearls Publishing, 2022.
[2] Myelodysplastic Syndrome (https://www.msdmanuals.com/professional/hematology-and-oncology/leukemias/myelodysplastic-syndrome-mds)
[3] ROLLISON, Dana E., et al. Epidemiology of myelodysplastic syndromes and chronic myeloproliferative disorders in the United States, 2001-2004, using data from the NAACCR and SEER programs. Blood, The Journal of the American Society of Hematology, 2008, 112.1: 45-52.
[4] MALCOVATI, Luca, et al. Diagnosis and treatment of primary myelodysplastic syndromes in adults: recommendations from the European LeukemiaNet. Blood, The Journal of the American Society of Hematology, 2013, 122.17: 2943-2964.
[5] AskMayoExpert. Myelodysplastic syndrome. Mayo Clinic; 2019
[6] Hoffman R, et al. Myelodysplastic syndromes. In: Hematology: Basic Principles and Practice. 7th ed. Elsevier; 2018. https://www.clinicalkey.com. Accessed Jan. 27, 2021.
[7] PEDERSEN-BJERGAARD, J., et al. Genetics of therapy-related myelodysplasia and acute myeloid leukemia. Leukemia, 2008, 22.2: 240-248.
[8] BEJAR, Rafael, et al. Clinical effect of point mutations in myelodysplastic syndromes. New England Journal of Medicine, 2011, 364.26: 2496-2506.
[9] ARBER, Daniel A., et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood, The Journal of the American Society of Hematology, 2016, 127.20: 2391-2405.
[10] GOLDBERG, Stuart L., et al. Incidence and clinical complications of myelodysplastic syndromes among United States Medicare beneficiaries. J Clin Oncol, 2010, 28.17: 2847-2852.
[11] Myelodysplastic syndromes (MDS) treatment side effects (https://bloodcancer.org.uk/understanding-blood-cancer/myelodysplastic-syndromes-mds/mds-treatment-side-effects/side-effects/)
[12] SABER, Wael; HOROWITZ, Mary M. Transplantation for myelodysplastic syndromes: who, when, and which conditioning regimens. Hematology 2014, the American Society of Hematology Education Program Book, 2016, 2016.1: 478-484.
[13] STERN, M., et al. Sensitivity of hematological malignancies to graft-versus-host effects: an EBMT megafile analysis. Leukemia, 2014, 28.11: 2235-2240.
[14] DE WITTE, T. J. M., et al. Intensive chemotherapy for poor prognosis myelodysplasia (MDS) and secondary acute myeloid leukemia (sAML) following MDS of more than 6 months duration: a pilot study by the Leukemia Cooperative Group of the European Organisation for Research and Treatment in Cancer (EORTC-LCG). 1995.
[15] RUUTU, Tapani, et al. Intensive chemotherapy of poor prognosis myelodysplastic syndromes (MDS) and acute myeloid leukemia following MDS with idarubicin and cytarabine. Leukemia research, 1997, 21.2: 133-138.
[16] NACHTKAMP, Kathrin, et al. Impact on survival of different treatments for myelodysplastic syndromes (MDS). Leukemia research, 2009, 33.8: 1024-1028.
[17] BARTENSTEIN, Matthias; DEEG, H. Joachim. Hematopoietic stem cell transplantation for MDS. Hematology/Oncology Clinics, 2010, 24.2: 407-422.
[18] Side Effects of a Bone Marrow Transplant (https://www.cancer.net/navigating-cancer-care/how-cancer-treated/bone-marrowstem-cell-transplantation/side-effects-bone-marrow-transplant-stem-cell-transplant)
[19] HORDYJEWSKA, Anna; POPIOŁEK, Łukasz; HORECKA, Anna. Characteristics of hematopoietic stem cells of umbilical cord blood. Cytotechnology, 2015, 67: 387-396.
[20] BARKER, Juliet N., et al. Availability of cord blood extends allogeneic hematopoietic stem cell transplant access to racial and ethnic minorities. Biology of Blood and Marrow Transplantation, 2010, 16.11: 1541-1548.
[21] KOPEC-SZLEZAK, J.; PODSTAWKA, U. Cord blood hematopoietic CD34+ cells. ACTA HAEMATOLOGICA POLONICA, 2001, 32.1: 61-70.
[22] CZAJKA, R., et al. The effect of umbilical cord blood cytokines on clonogenicity of hemopoietic stem cells isolated from umbilical cord blood. Ginekologia Polska, 1999, 70.12: 866-872.
[23] STOJKO, Rafał; WITEK, Andrzej. Umbilical cord blood–a perfect source of stem cells?. Ginekologia polska, 2005, 76.6: 491-497.
[24] SMOGORZEWSKA, E. M., et al. Purification of hematopoietic stem cells from human bone marrow and umbilical cord blood. Cent Eur J Immunol, 1997, 22: 232-239.
[25] DE LA GRANGE, Philippe Brunet, et al. Angiotensin II that reduces the colony-forming ability of hematopoietic progenitors in serum free medium has an inverse effect in serum-supplemented medium. Stem Cells, 2002, 20.3: 269-271.
[26] PORTER, David L.; ANTIN, Joseph H. Donor leukocyte infusions in myeloid malignancies: new strategies. Best practice & research Clinical haematology, 2006, 19.4: 737-755.
[27] SATO, A., et al. Unrelated cord blood transplantation after myeloablative conditioning in adults with advanced myelodysplastic syndromes. Bone marrow transplantation, 2011, 46.2: 257-261.
[28] GERDS, Aaron T., et al. Outcomes after umbilical cord blood transplantation for myelodysplastic syndromes. Biology of blood and marrow transplantation, 2017, 23.6: 971-979.
[29] HAHN, Theresa, et al. Significant improvement in survival after allogeneic hematopoietic cell transplantation during a period of significantly increased use, older recipient age, and use of unrelated donors. Journal of Clinical Oncology, 2013, 31.19: 2437.