Probiotics Applications in Type 2 Diabetes Treatment
Type 2 diabetes mellitus (T2DM) is characterized by increased fasting blood glucose (FBG) and glycosylated hemoglobin (HbA1c), indicating poor glucose uptake [1]. According to the American Diabetes Association (ADA) report, T2DM exhibits digestive disorders such as difficult stomach or intestinal clearance, gastric ulcers post-diabetes, constipation, diarrhea, bloating, and obesity [2,3]. Hence, the presence of digestive disorders is considered a stage in the development of T2DM. The pathogenesis of T2DM is complex and is also considered a chronic inflammatory disease [4]. Insulin resistance (IR) is a typical feature in most T2DM patients. T2DM is also associated with complications like coronary artery disease, atherosclerosis, kidney disease, heart disease, and foot injuries [5]. The causes of T2DM are multifaceted and linked to environmental exposure and genetics [1].
Currently, T2DM has become one of the most common diseases globally, and various treatment methods have been employed. However, some existing measures are not achieving the desired effectiveness. New promising strategies involve using probiotics directly or indirectly. Probiotics are microorganisms with health-improving properties. Current interventions for T2DM using probiotics have hypothesized that probiotics prevent T2DM in its growth, development, and symptoms. Research on T2DM in animal models uses both broad-spectrum probiotics at different levels and recombined probiotics. Probiotic therapy in T2DM shows promise and potential in the near future.
T2DM treatment and management by medication and changing lifestyle
Several current treatment modalities rely on lifestyle changes combined with the use of Eastern/Western medicines, providing certain levels of efficacy. However, they have both advantages and disadvantages in treating T2DM with some of the current medications. Many medications have been studied for their effectiveness using various approaches to control blood sugar levels. These medications can increase insulin production and utilization, inhibit sugar production and absorption, prevent glucose reabsorption, and increase glucose excretion in urine. Metformin and Vildagliptin are two standard medications widely prescribed in many T2DM clinics [6,7]. However, some individuals may be allergic to Metformin, causing adverse effects including persistent diarrhea even at low doses and Metformin-related lactic acidosis. The major drawback of Vildagliptin is joint pain. Insulin is also used as a supplement in the diet for T2DM. Subcutaneous insulin injections may cause skin rash, fat accumulation, or scarring at the injection site. Although the development of various insulin types has introduced new drugs, most require long-term continuous use and have some significant drawbacks.
Relationship between Microbiota and T2DM
Research suggests that the risk of developing T2DM may also be related to the gut microbiota. T2DM disrupts the gut microbiota, such as the gut bacteria Roseburia and F. prausnitzii, which have been detected in urine samples from patients (Figure 1) [8]. With the digestive symptoms of T2DM and the gut microbiota believed to be associated with the disease’s pathogenesis, the use of probiotics, a part of the gut microbiota, aids in T2DM treatment, as they are closely linked to the human diet, nutrition, and health. The gut microbiota, probiotics, and their impact on T2DM. Each individual carries about 1-2 kg of gut microbiota, representing several tens of billions of microorganisms comprising at least 1,000 different species. The gut microbiota affects various aspects of health and diseases [9].
These microorganisms play a crucial role in the permeability of the gut mucosa into the body’s immune system, which is an important factor in T2DM. Disruptions in the gut microbiota can be beneficial for energy absorption through diet, lipid production, and fat tissue growth, thereby slowing down the energy metabolism process, and leading to metabolic syndrome. Nowadays, adjusting the gut microbiota emerges as an interesting tool to prevent and/or treat metabolic disorders and gut microbiota disturbances related to obesity. Effective modulation of the gut microbiota can be achieved through probiotics or prebiotics. Probiotics are becoming increasingly popular as a functional food or dietary supplement as awareness of the health benefits of bacteria grows [10].
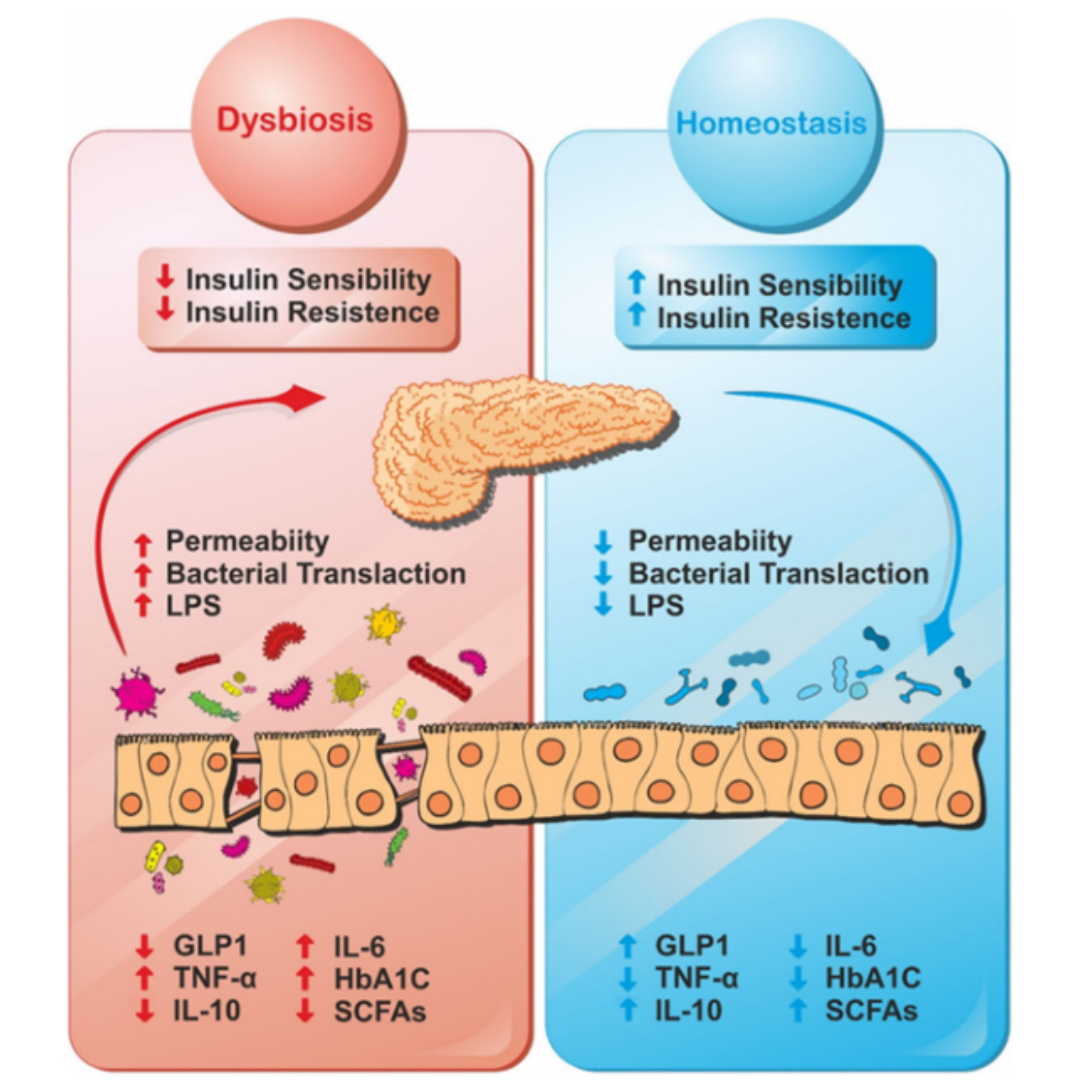
Figure 1: Gut microbiota in balance and bacterial disturbances due to diabetes.
The Mechanism and Clinical Trials of Using Probiotics for T2DM Treatment
Probiotics, comprising beneficial bacteria, and their intervention mechanisms in T2DM have been extensively studied. Many studies have been conducted on the use of probiotics as a dietary supplement in the prevention, intervention, and treatment of digestive disorders, including diabetes [11]. Generally, the beneficial effects of probiotics in T2DM intervention have been mediated by improving gut integrity, reducing systemic lipopolysaccharide (LPS) levels, enhancing incretin, and reducing endoplasmic reticulum (ER) stress. Probiotics may also treat diabetes by improving glucose absorption, regulating lipid metabolism, enhancing antioxidant capacity, and modulating gut microbiota and short-chain fatty acid composition [12]. Additionally, probiotics can reduce inflammatory responses, autoimmunity, and oxidative stress. Probiotics regulate the gut microbiota upon ingestion, modulate nutrient metabolism, and impact the immune response. Therefore, probiotic supplements contribute to reducing disease incidence, preventing and reversing inflammation and functional decline during the initiation, progression, and complications of T2DM.
Chronic metabolic inflammation is considered associated with increased insulin resistance, a hallmark of T2DM. The use of B. longum has reduced LPS, IL-1b, myeloperoxidase, and gut inflammatory activities in serum, closely related to gut and diabetes [13]. Studies have also indicated that probiotic interventions prevent the progression of T2DM by increasing glucose absorption and insulin sensitivity. Probiotics improve gut barrier function and increase secretion. Disease signs of T2DM include low-grade systemic inflammation and increased gut permeability. Gut bacteria are a significant cause of colonic inflammation. Dysbiosis of the gut microbiota leads to increased gut integrity, allowing bacterial toxins like LPS to enter circulation, causing inflammation, followed by insulin resistance and increased blood sugar.
Numerous clinical trials have registered interventions using probiotics for T2DM (https://clinicaltrials.gov). Studies have investigated the efficacy of treating diabetes with single-strain beneficial bacteria and/or multiple strains (combinations). Typically, patients are treated for 12 weeks using beneficial probiotics. Some studies have shown the supportive treatment efficacy of probiotics for T2DM. Probiotics help reduce insulin resistance, the ratio of low-density lipoprotein cholesterol to high-density lipoprotein cholesterol, and serum urea [14-16]. On the other hand, probiotics increase incretin, and insulin reduces insulin sensitivity, as well as certain enzymes and antioxidants in general.
Prospects of Probiotic Technology in T2DM Treatment
In summary, there are various perspectives on evaluating the effects of probiotics on T2DM, where some probiotic strains have been proven to reduce FPG and HbA1c in adults. Different beneficial bacterial strains have demonstrated effects on various forms of T2DM. Importantly, these beneficial strains differ greatly in both function and structure; for example, the Lactobacillus genus functions differently from other bacterial strains. The effect of probiotics on improving insulin resistance is related to enhancing gut microbiota and reducing LPS transport into circulation. Therefore, selecting probiotic strains may yield treatment outcomes in T2DM with safety and advantages.
References:
- Solis-Herrera, Carolina, Curtis Triplitt, Eugenio Cersosimo, and Ralph A. DeFronzo. “Pathogenesis of type 2 diabetes mellitus.” Endotext [Internet] (2021).
- Avalos, Danny J., Irene Sarosiek, Priyadarshini Loganathan, and Richard W. McCallum. “Diabetic gastroparesis: current challenges and future prospects.” Clinical and Experimental Gastroenterology (2018): 347-363.
- Azpiroz, Fernando, and Carolina Malagelada. “Diabetic neuropathy in the gut: pathogenesis and diagnosis.” Diabetologia 59, no. 3 (2016): 404-408.
- Herder, Christian, Eric J. Brunner, Wolfgang Rathmann, Klaus Strassburger, Adam G. Tabák, Nanette C. Schloot, and Daniel R. Witte. “Elevated levels of the anti-inflammatory interleukin-1 receptor antagonist precede the onset of type 2 diabetes: the Whitehall II study.” Diabetes care 32, no. 3 (2009): 421-423.
- Park, Tae Hyun, Min Sun Kim, and Dae-Yeol Lee. “Clinical and laboratory characteristics of childhood diabetes mellitus: a single-center study from 2000 to 2013.” Chonnam Medical Journal 52, no. 1 (2016): 64-69.
- Guarino, Elisa, Laura Nigi, Aurora Patti, Cecilia Fondelli, and Francesco Dotta. “Combination therapy with metformin plus vildagliptin in type 2 diabetes mellitus.” Expert Opinion on Pharmacotherapy 13, no. 9 (2012): 1377-1384.
- Bekiari, Eleni, Chrysoula Rizava, Eleni Athanasiadou, Konstantinos Papatheodorou, Aris Liakos, Thomas Karagiannis, Maria Mainou, Maria Rika, Panagiota Boura, and Apostolos Tsapas. “Systematic review and meta-analysis of vildagliptin for treatment of type 2 diabetes.” Endocrine 52 (2016): 458-480.
- Salgaço, Mateus Kawata, Liliane Garcia Segura Oliveira, Giselle Nobre Costa, Fernanda Bianchi, and Katia Sivieri. “Relationship between gut microbiota, probiotics, and type 2 diabetes mellitus.” Applied microbiology and biotechnology103 (2019): 9229-9238.
- Lallès, Jean-Paul. “Microbiota-host interplay at the gut epithelial level, health and nutrition.” Journal of Animal Science and Biotechnology 7 (2016): 1-8.
- Neef, Alexander, and Yolanda Sanz. “Future for probiotic science in functional food and dietary supplement development.” Current Opinion in Clinical Nutrition & Metabolic Care 16, no. 6 (2013): 679-687.
- Tonucci, Livia Bordalo, Karina Maria Olbrich Dos Santos, Leandro Licursi de Oliveira, Sonia Machado Rocha Ribeiro, and Hercia Stampini Duarte Martino. “Clinical application of probiotics in type 2 diabetes mellitus: A randomized, double-blind, placebo-controlled study.” Clinical nutrition 36, no. 1 (2017): 85-92.
- Simon, Marie-Christine, Klaus Strassburger, Bettina Nowotny, Hubert Kolb, Peter Nowotny, Volker Burkart, Fariba Zivehe et al. “Intake of Lactobacillus reuteri improves incretin and insulin secretion in glucose-tolerant humans: a proof of concept.” Diabetes care 38, no. 10 (2015): 1827-1834.
- Chen, Jin Jin, Ren Wang, Xiao-fang Li, and Rui-liang Wang. “Bifidobacterium longum supplementation improved high-fat-fed-induced metabolic syndrome and promoted intestinal Reg I gene expression.” Experimental Biology and Medicine 236, no. 7 (2011): 823-831.
- Firouzi, Somayyeh, Barakatun-Nisak Mohd-Yusof, Hazreen-Abd Majid, Amin Ismail, and Nor-Azmi Kamaruddin. “Effect of microbial cell preparation on renal profile and liver function among type 2 diabetics: a randomized controlled trial.” BMC complementary and alternative medicine 15, no. 1 (2015): 1-10.
- Tajabadi-Ebrahimi, M., N. Sharifi, A. Farrokhian, F. Raygan, F. Karamali, R. Razzaghi, S. Taheri, and Z. Asemi. “A randomized controlled clinical trial investigating the effect of synbiotic administration on markers of insulin metabolism and lipid profiles in overweight type 2 diabetic patients with coronary heart disease.” Experimental and Clinical Endocrinology & Diabetes 125, no. 01 (2017): 21-27.
- Bayat, Azade, Fatemeh Azizi-Soleiman, Motahar Heidari-Beni, Awat Feizi, Bijan Iraj, Reza Ghiasvand, and Gholamreza Askari. “Effect of Cucurbita ficifolia and probiotic yogurt consumption on blood glucose, lipid profile, and inflammatory marker in type 2 diabetes.” International journal of preventive medicine 7 (2016).