NK Cell Therapy in the Treatment of Acute Myeloid Leukemia
Disruption in the production of the body’s blood cells leads to the occurrence of Acute Myeloid Leukemia (AML), a rare form of blood cancer. These cells do not mature and divide properly, leading to abnormal growth and proliferation beyond control. As the disease progresses rapidly, early detection and treatment are crucial. According to the American Cancer Society, the United States alone is expected to have an estimated 20,000 new cases of AML and approximately 11,500 deaths from this condition in 2022 [1]. These numbers underscore the widespread impact of this disease. Despite advancements in AML treatment in recent years, relapse remains a significant concern. Hence, new treatment options are being researched to address unmet clinical needs. Among these novel therapies, immune-based natural killer (NK) cell therapy has emerged as a potential option to tackle these challenges [2]. NK cells are a type of immune cell in the body’s defense system capable of detecting and eliminating cancerous cells. With advancements in medical technology, there is hope that these new therapies will reduce the relapse rate and extend the lifespan of individuals with AML. However, treating this condition still requires high technical expertise, and early detection remains crucial for successful outcomes.
Characteristics of Acute Myeloid Leukemia and NK Cells in Blood
AML is termed as such because it affects a group of white blood cells called myeloid cells, which typically develop into various types of mature blood cells, such as red blood cells, white blood cells, and platelets [3]. AML occurs when a bone marrow myeloid cell undergoes changes in its genetic material or genes. Normally, DNA instructs cells to grow at a certain rate and die at a certain time. In AML, mutations instruct the bone marrow cell to continue growing and dividing. The bone marrow produces immature cells that develop into blast cells, a type of immature white blood cell [4]. These abnormal cells cannot function normally and may accumulate, overtaking healthy cells. Immune therapy has been recognized as a highly promising treatment strategy for various cancers, including AML [2]. In the body, immune cells and the immune system play crucial roles in detecting and eliminating infected or mutated cells.
The therapy based on natural killer (NK) cell immunity is one of the recent advancements in immune therapy, unleashing the immune suppression of NK cells to target various types of cancers [5]. With the development of NK cell therapy and technical advancements, the realm of immunotherapy for hematologic malignancies has expanded significantly in recent years. NK cells are the frontline defenders in the immune system against infections and malignant diseases [6]. These cells are crucial in both the innate and adaptive immune systems and are highly present in peripheral blood, lymph nodes, the liver, and bone marrow [7].
NK cells in AML
In acute myeloid leukemia (AML), the ability of cells to cause toxicity through NK intermediaries relies on “missing self-recognition” and “induced self-recognition” [8]. This function is regulated by a complex array of surface inhibitory receptors [e.g., killer cell immunoglobulin-like receptors (KIR), leukocyte immunoglobulin-like receptors (LIR), and CD94/NK group 2A (NKG2A)] and activating receptors [e.g., KIRs, CD94/NKG2C, NKG2D, and natural cytotoxicity receptors (NCR)], providing inhibitory and stimulatory signals [7]. There are two main sets of KIR genes, termed “A” and “B,” classified by distinct gene content. Type A primarily contains inhibitory genes and only one activating gene, KIR2DS4. Type B comprises both inhibitory and varying numbers of activating genes [9]. In AML, cancer cells can evade recognition through NK cell intermediaries due to abnormalities in NK and even leukocyte cells. The function of NK cells is tightly regulated by inhibitory and activating receptors, so an imbalance in their expression leads to functional disruptions [7].
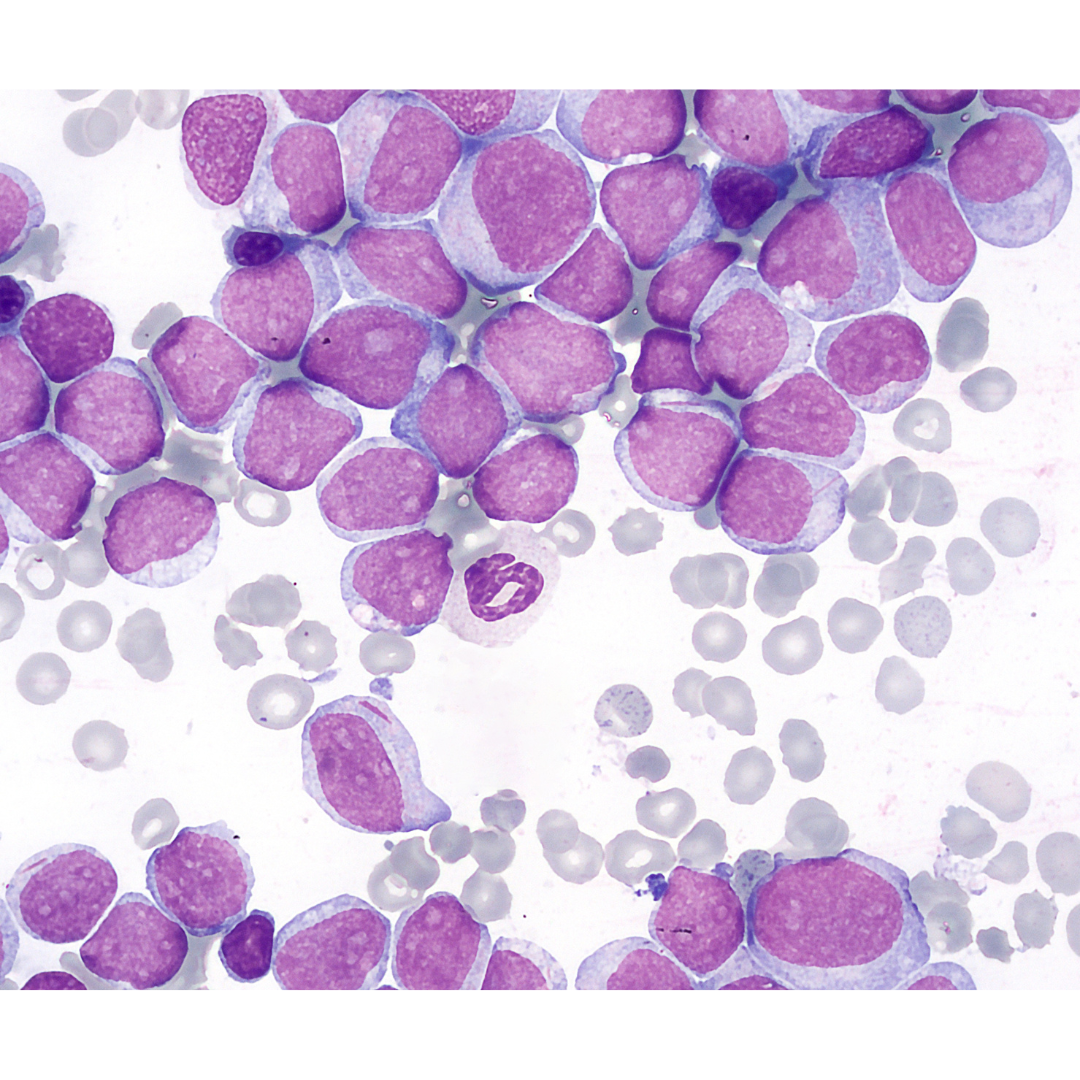
Acute myeloid leukemia (AML) is a cancer of the myeloid line of blood cells, characterized by the rapid growth of abnormal cells that build up in the bone marrow and blood and interfere with normal blood cell production. Symptoms may include feeling tired, shortness of breath, easy bruising and bleeding, and increased risk of infection. Occasionally, spread may occur to the brain, skin, or gums. As an acute leukemia, AML progresses rapidly, and is typically fatal within weeks or months if left untreated.
Studies indicate reduced expression of activating receptors like NKG2D, NCR, and the co-stimulatory molecule DNAX-1 (DNAM-1), as well as over-inhibition like KIR2DL2/L3 and NKG2A in AML patients compared to healthy counterparts [10]. The expression of NK receptors and their ligands on leukocytes, along with signals from the tumor microenvironment, is believed to impact clinical outcomes and relapse in AML patients [7]. Thus, the presence of dysfunctional NK cells in AML and their correlation with prognosis provide a basis for using NK cell-based immunotherapy to restore the cytotoxic capability of weakened NK cells against AML.
NK cell immunotherapy in acute myeloid leukemia and clinical trials
The strategy of transplanting NK cells relies on the beneficial effects of NK cells in allogeneic hematopoietic cell transplantation (HCT) settings. Allogeneic NK cell transplantation is considered a predictor of survival in recipients, especially from donors with a high content of KIR B genes [11]. The recovery of NK cells post-HCT correlates with improved outcomes, whereas decreased NK cell function could lead to relapse [12]. A study focusing on the effectiveness of IL-15 and IL-21-activated NK cells via HCT showed disease progression reduction in AML patients post-HCT but without infused NK cells [13]. Another study supplementing NK cells on days 2, 7, and 28 post-HCT through K562-mbIL21-41BBL-mediated cell transfer also proved effective in controlling AML relapse [14]. Notably, high expression of NKp30 on donor NK cells is predictive of high cytokine release and AML progression [14].
A dose-escalation study of NK cells demonstrated a close correlation between survival rates and the number of infused NK cells [15]. While this method yields a high AML remission rate, it is associated with mortality linked to GvHD. Therefore, conventional NK cell transplantation appears more than an ideal adjunctive and alternative therapeutic approach.
Miller and colleagues [16] pioneered mature NK cell transfer in AML patients without HCT, employing immune-suppressive conditioning with cyclophosphamide/fludarabine at high doses, proving to be a safe treatment direction, successfully inducing NK cell proliferation and activation in AML. Over the years, modifications to this approach have led to significant advancements, from donor selection based on inappropriate KIR ligands NK cell purification by CD3 depletion, followed by CD56 enrichment, to mitigate residual cell-induced side effects.
Transplanting NK cells conventionally is a feasible strategy for AML, not only aiding disease remission but also maintaining cytokine release capability. A phase I clinical trial assessed the feasibility and safety of transferring activated NK-92 cell lines from donors to AML patients. Additionally, a study demonstrated the feasibility of NK cells derived from hematopoietic stem progenitor cells (HSPC) isolated from umbilical cord blood (UCB) in a preclinical AML model [7]. The first study using cord blood-derived NKs to treat elderly AML patients showed enhanced proliferation and maturation in the body without NK cell-related toxicity [17].
Moreover, several methods, such as CAR-NK cell therapy, aim to modify NK cell genes in conventional transplantation to enhance efficacy. CAR-NK cell activity is extensively studied in various tumor models, but its applications in AML are relatively limited and primarily in preclinical stages [7]. Optimizing specific AML signatures as CAR-NK cell targets poses a significant challenge due to AML’s typified markers shared with normal hematopoietic stem cells (HSC). Experiences gained from exploring CAR-NK in AML treatment need further exploitation in the future, including optimizing CAR-NK cell targets and structures, as well as investigating suitable patients for this immunotherapy.
An initial clinical study on allogeneic transplantation post-NK cell expansion using mismatched donors to treat poor-prognosis AML patients with immune suppressive chemotherapy, including cyclophosphamide and methylprednisolone, showed complete remission in over 25% of AML patients, with a higher complete remission rate among mismatched donors, indicating the potential interaction of NK cells. A clinical trial in 2009 examining the impact of high-dose (more than 10–20 times higher than previous doses) HCT from related donors and HCT for chemotherapy-resistant AML patients showed significant disease progression reduction post-treatment. Although only a third of patients achieved complete remission after treatment, it was significant as these patients were chemotherapy-resistant, and their cancers were untreatable through conventional therapies.
A clinical trial treating pediatric AML patients via conventional NK cell transplantation post-expansion recorded minimal effectiveness, suggesting that intermediate or standard pediatric AML stages might not be amenable to this form of treatment [20].
A clinical trial using HLA-mismatched cord blood-derived CAR-NK cells to treat relapsed and refractory pediatric AML showed complete remission in 73% of patients [21]. All patients responded rapidly to CAR-NK therapy without significant adverse effects. The proliferative capacity of CAR-NK cells was monitored, and characteristics were sustained for up to 12 months post-transplantation [21].
Although certain methods have shown efficacy, further clinical trials are needed to assess the safety and efficacy of NK cell transplantation, exploring optimal NK cell dosages, sources, optimal timing concerning HCT, and potential combined therapies.
References:
[1] EICHHORST, Barbara, et al. First-line chemoimmunotherapy with bendamustine and rituximab versus fludarabine, cyclophosphamide, and rituximab in patients with advanced chronic lymphocytic leukemia (CLL10): an international, open-label, randomised, phase 3, non-inferiority trial. The lancet oncology, 2016, 17.7: 928-942.
[2] FARKONA, Sofia; DIAMANDIS, Eleftherios P.; BLASUTIG, Ivan M. Cancer immunotherapy: the beginning of the end of cancer?. BMC medicine, 2016, 14.1: 1-18.
[3] AskMayoExpert. Acute myeloid leukemia (adult). Mayo Clinic; 2020.
[4] Hoffman R, et al. Clinical manifestations and treatment of acute myeloid leukemia. In: Hematology: Basic Principles and Practice. 7th ed. Elsevier; 2018.
[5] FANG, Fang; XIAO, Weihua; TIAN, Zhigang. NK cell-based immunotherapy for cancer. In: Seminars in immunology. Academic Press, 2017. p. 37-54..
[6] SPITS, Hergen, et al. Innate lymphoid cells—a proposal for uniform nomenclature. Nature reviews immunology, 2013, 13.2: 145-149.
[7] XU, Jing; NIU, Ting. Natural killer cell-based immunotherapy for acute myeloid leukemia. Journal of Hematology & Oncology, 2020, 13.1: 1-20.
[8] LJUNGGREN, Hans-Gustaf; KÄRRE, Klas. In search of the ‘missing self’: MHC molecules and NK cell recognition. Immunology today, 1990, 11: 237-244.
[9] HANDGRETINGER, Rupert; LANG, Peter; ANDRÉ, Maya C. Exploitation of natural killer cells for the treatment of acute leukemia. Blood, The Journal of the American Society of Hematology, 2016, 127.26: 3341-3349.
[10] COSTELLO, Régis T., et al. Defective expression and function of natural killer cell–triggering receptors in patients with acute myeloid leukemia. Blood, The Journal of the American Society of Hematology, 2002, 99.10: 3661-3667.
[11] RUGGERI, Loredana, et al. Donor natural killer cell allorecognition of missing self in haploidentical hematopoietic transplantation for acute myeloid leukemia: challenging its predictive value. Blood, The Journal of the American Society of Hematology, 2007, 110.1: 433-440.
[12] PITTARI, G., et al. Early evaluation of natural killer activity in post-transplant acute myeloid leukemia patients. Bone marrow transplantation, 2010, 45.5: 862-871.
[13] CHOI, Inpyo, et al. Donor-derived natural killer cells infused after human leukocyte antigen–haploidentical hematopoietic cell transplantation: a dose-escalation study. Biology of Blood and Marrow Transplantation, 2014, 20.5: 696-704.
[14] CIUREA, Stefan O., et al. Phase 1 clinical trial using mbIL21 ex vivo–expanded donor-derived NK cells after haploidentical transplantation. Blood, The Journal of the American Society of Hematology, 2017, 130.16: 1857-1868.
[15] LEE, Dean A., et al. Haploidentical natural killer cells infused before allogeneic stem cell transplantation for myeloid malignancies: a phase I trial. Biology of Blood and Marrow Transplantation, 2016, 22.7: 1290-1298.
[16] MILLER, Jeffrey S., et al. Successful adoptive transfer and in vivo expansion of human haploidentical NK cells in patients with cancer. Blood, 2005, 105.8: 3051-3057.
[17] DOLSTRA, Harry, et al. Successful transfer of umbilical cord blood CD34+ hematopoietic stem and progenitor-derived NK cells in older acute myeloid leukemia patients. Clinical Cancer Research, 2017, 23.15: 4107-4118.
[18] MILLER, Jeffrey S., et al. Successful adoptive transfer and in vivo expansion of human haploidentical NK cells in patients with cancer. Blood, 2005, 105.8: 3051-3057.
[19] CHOI, Inpyo, et al. Donor-derived natural killer cells infused after human leukocyte antigen–haploidentical hematopoietic cell transplantation: a dose-escalation study. Biology of Blood and Marrow Transplantation, 2014, 20.5: 696-704.
[20] NGUYEN, Rosa, et al. A phase II clinical trial of adoptive transfer of haploidentical natural killer cells for consolidation therapy of pediatric acute myeloid leukemia. Journal for ImmunoTherapy of Cancer, 2019, 7: 1-7..
[21] LIU, Enli, et al. Use of CAR-transduced natural killer cells in CD19-positive lymphoid tumors. New England Journal of Medicine, 2020, 382.6: 545-553.